70 YEAR OLD MALE WITH FLANK PAIN AND FEVER
This is an online E logbook to discuss our patients' de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from the available global online community of experts intending to solve those patients clinical problems with the collective current best evidence-based inputs. This e-log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box are welcome.


 USG ABDOMEN:
USG ABDOMEN:

 Bulky right kidney
Bulky right kidney

CHEIF COMPLAINTS:
Patient came with c/o of flank pain and fever since 5 days
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 1 month back then developed flank pain which is insidious in onset and gradually progressive which is of dragging type
Then developed fever and burning micturition 7 days back
For burning micturition he used citralka syrup and subsided and he stopped using medication and again started burning micturition
H/o increased frequency of urination +
(He urinates for every 20 min)
H/o urgency of urination +
No h/o Hematuria,
No h/o suprapubic pain
No h/o dribbling of urine
Fever which aggrevates at night and subsides automatically and associated with chills and subsides in the morning automatically
H/o nausea since 5 days
No h/o chest pain,palpitation,sob,sweating
PAST HISTORY:
K/c/o HTN since 1 year used medication(unknown medication) for 2 months and stopped due to controlled blood pressure
K/c/o DM for 2 year used medication (unknown medication)for 3 months and stopped due to controlled blood sugars
Not a k/c/o TB,ASTHMA, EPILEPSY,THYROID DISORDERS,CVA,CAD
ALLERGIC HISTORY:
No history of any kind of allergies of food or drug
PERSONAL HISTORY:
Appetite: decreased
Sleep:adequate
Bowel and bladder regular
Addictions:He stopped taking alcohol 1 year back
Before 1 year he used to drink for every 1 month (90ml at a time)
He used to be a smoker 20 years back
FAMILY HISTORY:
Not significant
GENERAL EXAMINATION:
patient is conscious/coherent/cooperative
No pallor,icterus,cyanosis,clubbing,lypmaphadenopathy,edema
SYSTEMIC EXAMINATION:
cvs:s1 and s2 +
Rs:Bae+nvbs
P/A :
Inspection:
abdomen distended
No scars sinuses present
Umbilical inverted
Palpation:
soft and tenderness in right lumbar region
Right loin tenderness+
Fluid thrill +
Percussion:
Shifting dullness +
Auscultation:
Bowel sounds +
CNS:
no focal neurological deficits
Provisional diagnosis:
FEVER UNDER EVALUATION
K/C/O DM ,HTN
INVESTIGATIONS:-
DATE :- 8/2/24
BT - 2min 00sec
CT - 4 min 30 sec
PT 1.20 sec
Malaria --ve
Dengue -ve
Widal test -ve
Urine for ketone bodies - +ve
CBP:-
Hb:- 12.1 gm/dl
TLC :- 8,300 cells N-85/L-10/E-2/M-3/B-0
PLT - 1.20 lakhs
CUE:-
Alb- 3+
Sugars - 4+
Pus cells - 4-6cells
epi:- 2-4cells
RFT:-
Serum creatinine:- 1.2 mg/dl
Serum Na :-135 mEq/L
Serum K :- 3.5 mEq/L
Serum cl :-98
Serum ca -1.21
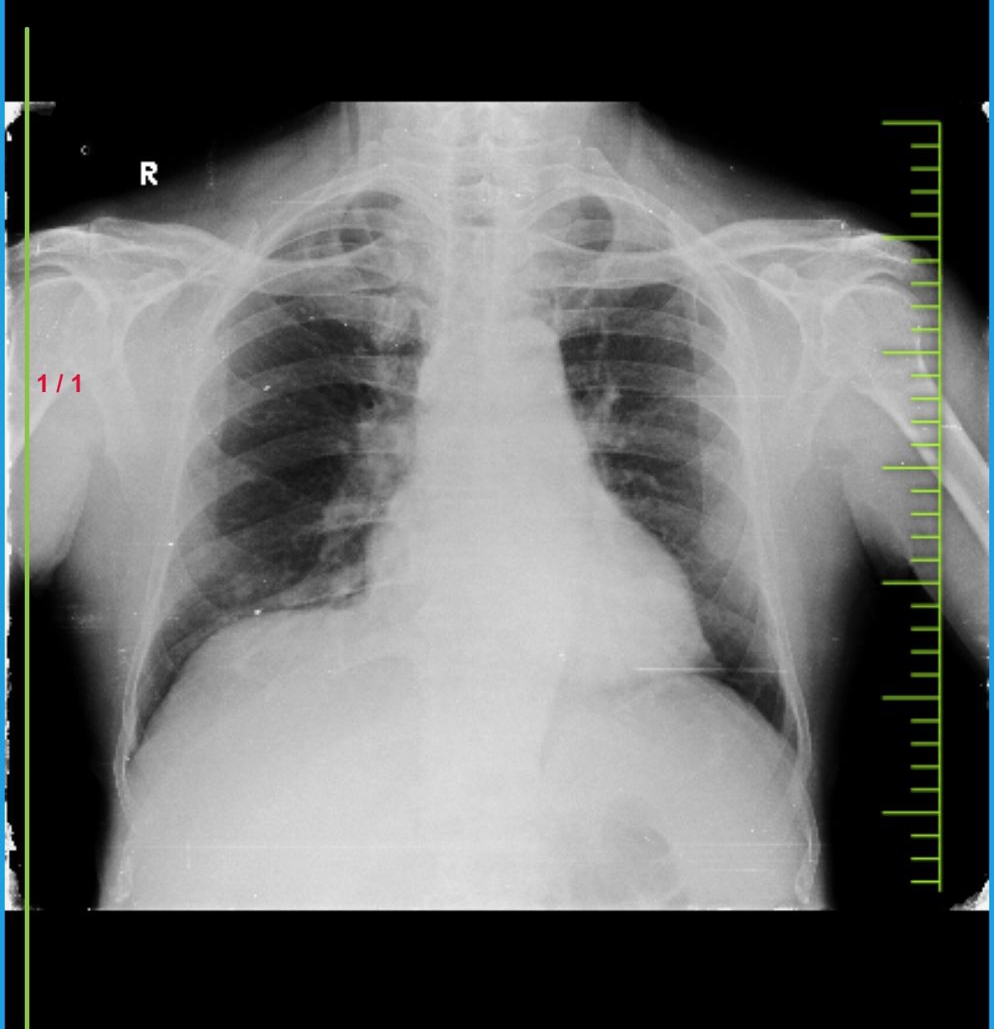
CHEST XRAY:
8/2/24
ECG:
BULKY RIGHT KIDNEY WITH HYPERECHOGENICITY
E/O FEW CYSTS NOTED IN LEFT KIDNEY LARGEST MEASURING 11 X 9 MM IN UPPER POLE
Bulky right kidneyIMPRESSION:
ACUTE RIGHT PYELONEPHRITIS
GRADE 1 PROSTATOMEGALY
GRADE 1 FATTY LIVER
LEFT RENAL CORTICAL CYSTS
MILD SPLENOMEGALY
2D ECHO :
SINUS ARRYTHMIA
CONCENTRIC LVH
MODERATE AR,MILD MR,MODERATE TR
MILD CALCIFIED AV,THICKENED AV
EF =63
GOOD LV SYSTOLIC FUNCTION
DIASTOLYIC DYSFUNCTION+
NO PAH
MILD MA +
IVC SIZE (1.18CMS) COLLAPSING
https://youtube.com/shorts/5TFi6jZ1sDk?si=FMBt4bUbYNcJ6tWt
DIAGNOSIS :-
DIABETIC KETOSIS
ACUTE PYELONEPHRITIS
K/C/O HTN AND DM
9/2/24:
FBS -129
Serum NA:135
SERUM K :3.5
SERUM CL :98
SERUM CA : 1.23
SERUM OSMOLALITY: 275
URINE KETONE BODIES :+VE
DOA - 8/2/24
S :-
Fever at 10:30am
Stools not passed
O:
Pt is c/c/c
Bp - 110/80 mmhg
Pr- 81 bpm
RR :- 18 cpm
Grbs :- 174 mg/dl
Cvs - S1 S2 heard no murmurs
Rs - Bae+ Nvbs
P/A :
Soft and tenderness present in right lumbar region
CNS:- NFND
A:
-DIABETIC KETOSIS
-ACUTE PYELONEPHEITIS
-K/C/O DM AND HTN
P :- 1 IVF 2 Ns @ 100 ml/ hr
2 INJ MONOCEF 1g IV / bd
3 INJ NEOMOL 1g IV /soa IF TEMP > 101F
4 TAB AMLONG 5.mg po /OD
5 INJ HAT sc/TID ACC TO GRBS
6 GRBS MONITOR EVERY HOURLY
INJ KCL 1amp IN 500 ml NS OVER 5 HOURS
10/2/24
Hb:13.1
Tlc:9,400
N/L/E:88/6/0
Pcv:38.4
Mcv:81.5
Serum NA:134
SERUM K :3.5
SERUM CL :99
SERUM CA : 1.13
DOA - 8/2/24
S :-
2 fever spikes at 11:30 pm and 6:00am
Stools not passed
O:
Pt is c/c/c
Temp: 97.6f
Bp - 140/80 mmhg
Pr- 102bpm
RR :- 22 cpm
Grbs :172mg/dl
Cvs - S1 S2 heard no murmurs
Rs - Bae+ , crepts at right axillary area and right mammary area
P/A-Inspection:
abdomen distended
No scars sinuses present
Umbilical inverted
Palpation:
soft and tenderness in right lumbar region
Right loin tenderness+
Fluid thrill +
Percussion:
Shifting dullness +
Auscultation:
Bowel sounds +
CNS:- NFND
A:
-DIABETIC KETOSIS
-ACUTE PYELONEPHEITIS
-K/C/O DM AND HTN
P :- 1 IVF 2 Ns @ 100 ml/ hr
2 INJ MONOCEF 1g IV / bd
3 INJ NEOMOL 1g IV /sos
4 TAB AMLONG 5.mg po /OD
5 INJ HAT sc/TID ACC TO GRBS
6 GRBS MONITOR EVERY HOURLY
7 SYRUP CREMAFFIN PLUS 15ml PO/HS
8 NEB WITH DUOLIN AND BUDECORT 6th HOURLY
11/2/24:


Comments
Post a Comment